
With almost 360 degrees of motion (across several planes), the shoulder is by far the most mobile joint in the human body. It has achieved this generous range of motion through the sacrifice of stability and a reliance on active and passive restraints (muscle, capsule and ligaments) over bony concurrency. This makes the shoulder one of the most complex joints with more than a dozen muscles working together to raise, twist and move the arm.
Osteology: (the bones involved)
The three main bones of the shoulder are the humerus (the upper arm) the scapula (shoulder blade), and the clavicle. Often the clavicle is the underappreciated, but, as it represents the only true bony connection of the shoulder girdle to the axial skeleton, it deserves recognition. When looking at it from a physical therapy perspective, a dysfunctional clavicle can cause the entire system to break down.
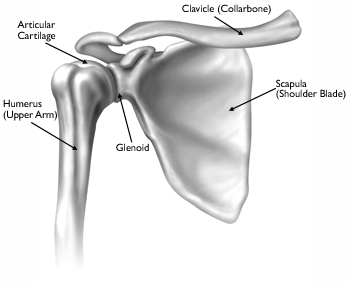
anterior view of the bones of the shoulder complex
The clavicle runs from the sternum across to the acromion (tip of the scapula) and comprises two joints of the shoulder girdle: the sternoclavicular (SC) joint and the acromioclavicular (AC) joint.
The scapula is located on the back of the thorax (along the mid back). The scapula is triangular in shape and serves as an attachment point for many of the muscles required for shoulder motion. At the lateral edge, lies the glenoid fossa - the "socket" of the glenohumeral joint. Along the midpoint of the scapula runs the scapular spine, which ends laterally along the top and the front of the shoulder via a projection known as the acromion. The acromion can be thought of as the "roof" or “arch” over the glenohumeral joint. In some texts you may even see it describes as "an arch." It serves a protective function (shielding the humeral head and joint space) and as an attachment point for several of the muscles that act on the scapula and the glenohumeral joint.
The humerus is the upper arm bone. The humeral head is the "ball" portion of the glenohumeral joint and meets with the concave glenoid fossa just under the acromion.
Beyond these three bones, it is important to recognize that the ribs, the thoracic vertebrae, the cervical vertebrae and the pelvis all act on the shoulder through muscular and fascial attachments. If any of these bones and joints is not moving well or is injured, the shoulder's complex mobility begins to lessen.

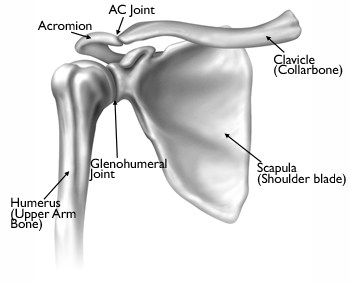
anterior view of the four joints that make up the shoulder complex
The four joints of the shoulder complex:
1. The glenohumeral joint
2. The sternoclavicular joint
3. The acromioclavicular joint
4. The scapulothoracic joint
The glenohumeral (GH) joint:
anterior view of the glenohumeral joint
The articulating surface of the scapula, called the glenoid, meets the head of the humerus to form the glenohumeral joint (GH joint). It is a true synovial joint (synovial fluid within a fibrous capsule) and articular cartilage covers the head of the humerus and face of the glenoid to provide cushioning and a smooth surface for joint gliding. As the humeral head is much larger than the glenoid (think a tennis ball on a quarter), the arm has a tremendous ability to move, but is inherently unstable. This cartilage helps guide movement and protects the joint surfaces. As with any joint, the GH joint is susceptible to injury and general "wear and tear."
Due to the lack of congruence between the humeral head and the glenoid, a ring of fibrous cartilage surrounding the glenoid called the labrum stabilizes the joint. This makes the glenoid seem larger and increases stability, while being flexible and elastic enough to stretch and allow the shoulder to maintain its almost 360 degrees of mobility. The labrum is commonly injured, and like the meniscus of the knee, does not heal itself well without outside intervention (surgery/rehabilitation).
The sternoclavicular joint:
The sternoclavicular (SC) joint is composed of the medial end of the clavicle and its attachment on the sternum. It is a synovial joint (cartilage on both surfaces and fluid between), with a fibrocartilage disk between the bones to improve congruency. This joint is extremely strong, with ligamentous support that does not dislocate easily (fracture of the clavicle is more common). The functions of the SC joint include:
· Anchoring the clavicle and the shoulder girdle to the torso/thorax
· Acting as a pivot point about which the clavicle moves/rotates to allow for motions of the shoulder complex.
There are no muscles that act directly on the SC joint, but through their actions on the clavicle and the surrounding ribs, some can assist in motion of the clavicle. The SC joint has three paired directions of motion (aka degrees of freedom)
1. Inferior and superior glide
2. Anterior and posterior glide
3. Axial rotation (up and down around the axis of the clavicle)
When the SC joint becomes dysfunctional (most often hypomobile or “stiff”), it causes more stress on the remaining joints of the shoulder complex and can lead to their accelerated degeneration. With chronic or insidious shoulder injuries (a.k.a. “It just started hurting and I can’t think of a reason”), often the SC joint is dysfunctional and needs to be evaluated.
The acromioclavicular joint:
The acromioclavicular (AC) joint is formed by the lateral edge of the clavicle and its intersection with the acromion process of the scapula. It is a synovial joint (cartilage on both surfaces and fluid between). The primary functions of the AC Joint are:
- To allow the scapula additional range of rotation on the thorax (rib cage)
- Allow for adjustments of the position of the scapula (tipping and internal/external rotation) such that it can follow the motion of the torso and ribs with movement.
- Allow for the transmission of forces from the upper extremity to the clavicle.
The AC joint and the SC joint work together to allow for motions of the scapula and shoulder. At the AC joint, the specific directions of movement available include:
1. Inferior/superior glide
2. Internal/external rotation (about the axis of the clavicle)
The joint capsule, ligaments surrounding the joint and the adjacent muscles all work together to provide stability and to keep the clavicle in contact with the acromion process of the scapula. However, even with multiple types of supports, the AC joint lacks congruency and is relatively weak. AC joint sprains are common (caused by falling on an outstretching hand or sudden traction to the shoulder) and represent a significant source of chronic shoulder problems. Beyond that, the AC joint begins to degenerate in our 20’s and by the early 60’s, the joint space is markedly narrowed in a large percentage of the healthy population.
The scapulothoracic joint:
The scapulothoracic (ST) joint is not a true synovial joint, however it is a complex connection that is essential with all shoulder motion. It is an articulation of the scapula with the posterior thoracic wall, and depends on the integrity of the acromioclavicular (AC) and sternoclavicular (SC) joints. In fact, all three joints must move together in perfect synchrony for the shoulder to remain mobile, stable and healthy.
When the arm is raised, the scapula (shoulder blade) moves on the thorax to allow for the wide range of pain-free and uninterrupted motion at the shoulder. As the timing of this motion is complicated and reliant on many muscles working together, many shoulder problems begin with a slight variation in this rhythm (known as “scapulothoracic rhythm”).
The motions of the ST joint include:
1. Anterior/posterior tilt
2. Superior/inferior glide
3. Protraction (gliding apart from one another) and retraction (pinching your shoulder blades together)
4. Upward/downward rotation (think of the pivot as being the center of the scapula as seen from the back; almost clockwise/counterclockwise motion)
Ligaments/Tendons of the Shoulder:
Ligaments connect the bones of the shoulder to one another. These are the passive stabilizers (meaning that they work even without the muscles to keep the joint intact). There are several ligaments at each of the joints (the SC, the AC and the glenohumeral). In the case of the glenohumeral joint, the ligaments blend with the joint capsule - the fibrous covering that holds joint fluid (synovial fluid) in. This adds stability and strength to the structure.
There are also tendons around the shoulder that connect muscle to bone and allow for movement. Their placement serves to further stabilize the joint. Because of their connection to muscles, tendons stabilize the joint actively (as compared to what the ligaments do passively) when the muscles contract. One of the most visible and important tendons in this area is the biceps tendon which attaches the biceps muscle to the shoulder and helps to stabilize the front (anterior) portion of the shoulder joint. In many injuries of the shoulder, this tendon can become inflamed or torn.
The Rotator Cuff:
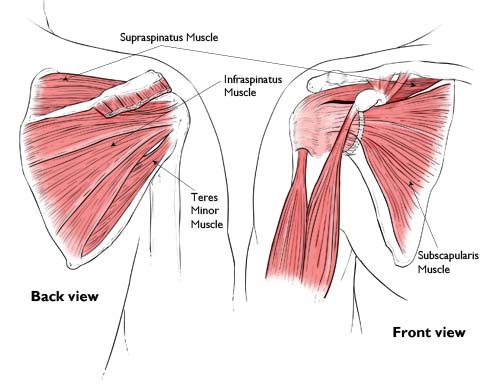
The rotator cuff is composed of four small, short muscles that originate on the scapula and pass around the shoulder where their tendons fuse together and attach on the humerus. Known as the "SITS" muscles, they are:
- Supraspinatus
- Infraspinatus
- Teres minor
- Subscapularis
These muscles have two main functions. First, they stabilize the joint and help center the humeral head in the glenoid fossa during all motion (basically they balance that tennis ball on that quarter). Second, they control rotation of the shoulder and allow for complex movements through diagonals and multiple planes (think of reaching into the cabinet or behind you in the car).
Warning: Unique Ideas Ahead - Beyond those two functions, it is the personal opinion of this acrobatic physical therapist that the rotator cuff takes on a third function in weight bearing activities. (i.e. body support positions like push up position or handstands; and pull-ups or hanging skills.) In these situations, the direction of pull changes from open kinetic chain to closed kinetic chain. This means that the distal bone (the one farther from the center of the body) now moves on the proximal one (the one closer to the center). That means that the humerus now rolls/moves on the glenoid. This increases the force on the RTC (rotator cuff) exponentially because now it has to carry the weight of the head, torso and legs (rather than the arms). To better visualize it, the shoulder has now taken on the role that the hip normal takes in upright walking, so the RTC is analogous to the gluteal muscles. In this role, the rotator cuff acts as a stabilizer and as a prime mover of a much larger weight - a dual role that puts it at a higher risk of injury. (And now back to the standard anatomical knowledge…)
Other musculature:
Many other muscles that directly connect the shoulder with the surrounding skeleton are also worth noting. Normally, most articles will reference 8 (including the 4 rotator cuff muscles). Ha! If only it were that simple. The more extensive list includes:
- The biceps
- The triceps
- The pectoralis major
- The pectoralis minor
- The latissimus dorsi
- The serratus anterior
- The serratus posterior superior
- The rhomboid major
- The rhomboid minor
- The upper, middle and lower trapezius
- The levator scapula
- The deltoid (anterior, middle and posterior)
- The coracobrachialis
- The subclavius
- The anterior, middle and posterior scalene (through an indirect effect)
- The sternocleidomastoid (through an indirect effect)
But wait - there's more:
Within the shoulder also lies a structure called the "brachial plexus." This is the collection of nerves that merge after exiting the neck that then travel down the arm, providing sensation and muscular innervation to all the muscles from the shoulder to the hand.
It’s important to note that nerves stretch and glide with movement too - and if they become compressed (by bone, fascia or muscle) they can limit mobility and cause problems for the remaining structures. So, this nerve bundle is a big deal and should the brachial plexus become compressed or damaged, it can significantly alter shoulder motion and can leave someone with permanent injury in the arm/hand.
References:
1. Conway, A.M. (1961). Movements at the sternoclavicular and acromioclavicular joints. Phys Ther Rev. 41: 421-432.
2. Dutton, M. (2008). Orthopaedic: Examination, evaluation, and intervention (2nd ed.). New York: The McGraw-Hill Companies, Inc.
3. Inman, V.T., Saudners, J.B., Abbot, L.C. (1996). Observations of the function of the shoulder joint. 1944. Clin Orthop Relat Res. 3-12.
4. Kibler WB. The role of the scapula in athletic shoulder function. Am J Sports Med 1998; 26:325-337
5. Levangie, P.K. and Norkin, C.C. (2005). Joint structure and function: A comprehensive analysis (4th ed.). Philadelphia: The F.A. Davis Company.
6. McQuade K, Smidt G: Dynamic scapulohumeral rhythm: The effects of external resistance during elevation of the arm in the scapular plane. J Orthop Sports Phys Ther 1998; 27:125–133.
7. Neumann DA. Kinesiology of the musculoskeletal system: Foundations for Physical Rehabilitation.2nd Ed. Elsevier Health Sciences; 2009
8. Teece, R.M., Lunden, J.B., Lloyd, A.S., Kaiser, A.P., Cieminski, C.J., Ludewig, P.M. (2008). Three-dimensional acromioclavicular motions during elevation of the arm. J Orthop Sports Phys Ther. 38(4), 181-90.